Microscopy Images
The thin basement membrane lesion is the underlying morphologic change in most families with benign familial hematuria and may also be seen in sporadic cases of hematuria. Many of these kindreds are carriers of autosomal recessive Alport syndrome.
Patients show persistent microscopic hematuria, often with intermittent macroscopic hematuria. Of patients biopsied for persistent isolated hematuria, thin basement membranes may be present in 20% to 25%.
Prognosis is generally benign, with slight increased risk of chronic kidney disease in carriers of Alport syndrome.
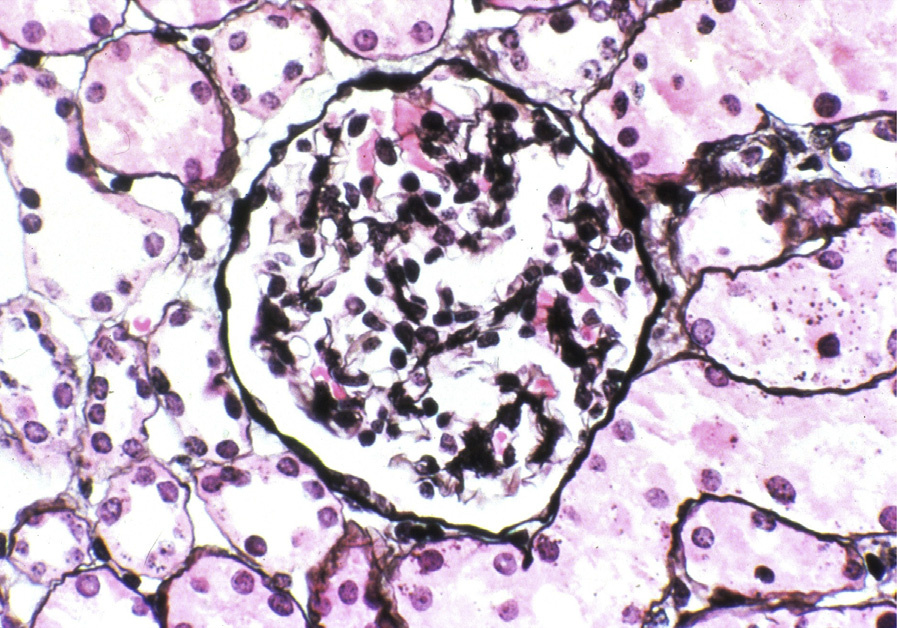
Light microscopy: No specific lesions.
Immunofluorescence microscopy: No immune complexes are seen, with normal staining for type IV collagen alpha 3, 4, 5 in carriers of autosomal recessive Alport. Carriers for X-linked Alport show mosaic staining along glomerular basement membranes (GBMs) for type IV collagen alpha 3 and 5.
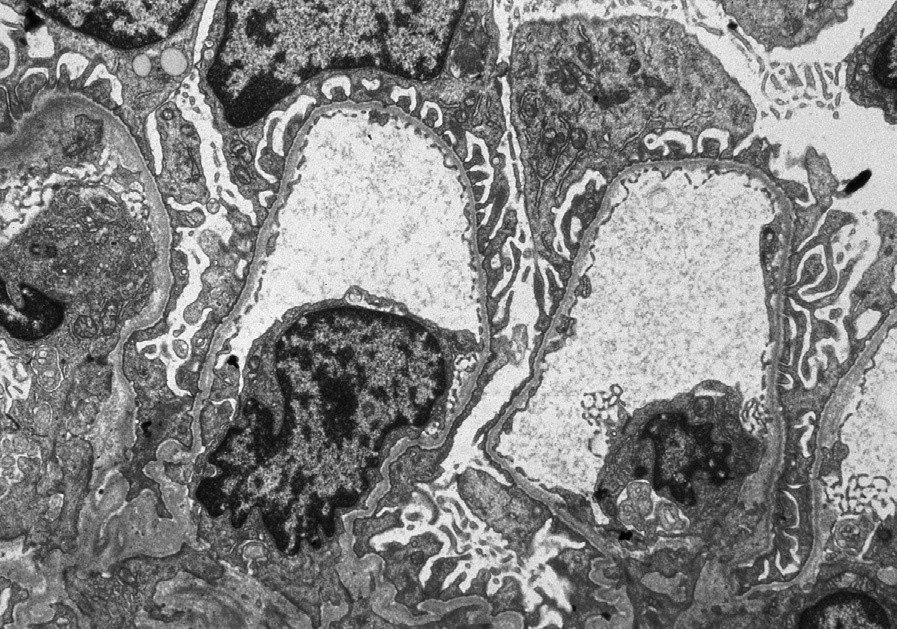
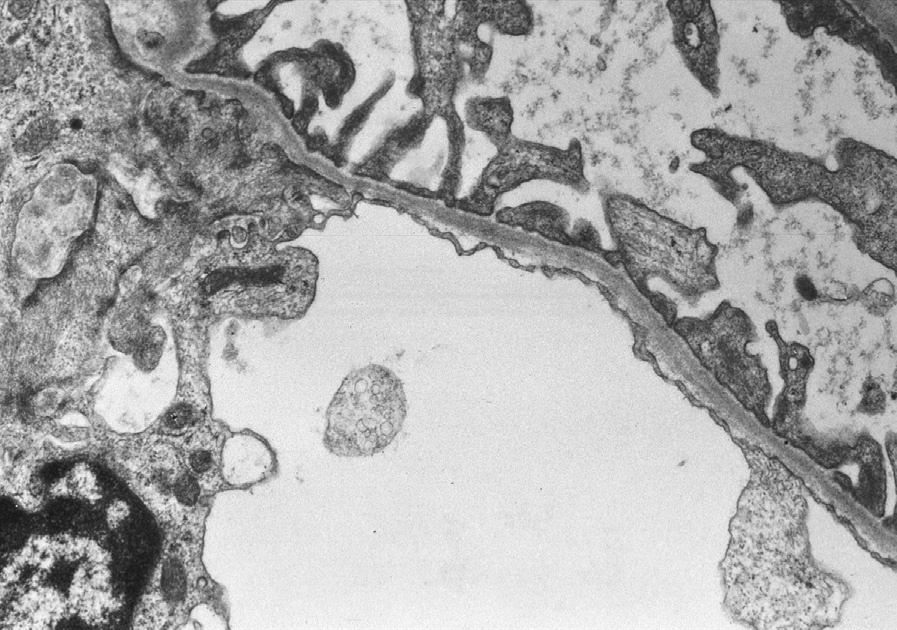
Electron microscopy: The lamina densa of the GBM shows marked and extensive thinning in a majority of capillary loops, compared to age-matched controls, as GBM normally increases in thickness with age. A 250 nm lower limit of normal is suggested in adults, with normal thickness in our laboratory around 110 nm at 1 year of age to 222 6 14 nm by age 7.
Many patients with thin basement membrane lesion and family history of hematuria have carrier status for mutations of type IV collagen alpha 3 or 4.
Thin GBMs are seen early in Alport, in the carrier state of X-linked Alport, and the carrier states of autosomal recessive Alport. Clinical history, staining for type IV collagen chains, and genetic testing can differentiate between these possibilities.